
Glaucoma and Uveitis
Glaucoma is the name given to a number of conditions in which the optic nerve is damaged where it leaves the eye. This type of damage has characteristic features and effects on vision. There are many types of glaucoma, but for the purposes of this article we shall concentrate on those types that are associated with uveitis.
Up to 20% of patients
with uveitis will develop glaucoma. Glaucoma caused by uveitis, is
called a secondary glaucoma. In uveitis patients, glaucoma is normally
the result of a rise in pressure inside the eye (intraocular pressure).
This will be explained below after a look at the parts of the eye
involved. At this point it is worth pointing out that, often, raised
intraocular pressure (IOP) is taken to be the same thing as glaucoma.
This is not accurate, they are actually quite different. It is just
that a raised IOP will lead to glaucoma if not treated.
Anatomy of the eye in relation to Glaucoma
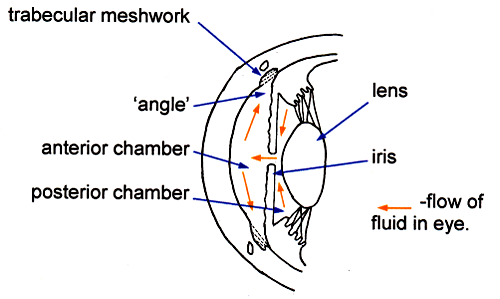
The space in front of the lens contains watery fluid, the aqueous and behind the lens, the rest of the eye is filled with a clear jelly, the vitreous. The watery compartment is divided into two, the anterior chamber, which is in front of the iris and the posterior chamber behind the iris but in front of and at the side of the lens. (The vitreous compartment is often mistakenly thought to be the posterior chamber). Watery fluid is secreted into the posterior chamber by special cells covering the inner surface of the ciliary body and passes through the pupil into the anterior chamber where, in the angle of the anterior chamber, it is normally able to drain through a special sieve-like tissue called the trabecular meshwork leading to a circular drainage canal from which it passes back into the blood stream (trabecular flow). A balance between the fluid entering and leaving the eye determines the pressure within it - the intraocular pressure. This pressure maintains the shape of the eye, a little like air pressure in a balloon.Raised Intraocular pressure and glaucoma
There are several different ways in which this pressure can be raised and it can happen slowly (chronic) or occasionally quickly (acute). The upper limit of 'normal' is generally taken to be 21 mmHg. and is measured very simply. If the IOP is above 21mmHg but there is no damage to the optic nerve then the term ocular hypertension is used.The increased pressure, in time, will damage the end of the optic nerve by affecting the blood supply to the nerve or by directly damaging the nerve endings .. It is this damage which is called glaucoma. The damage to the optic nerve has characteristic effects on the vision. This is why it is important to be able to distinguish between a raised IOP and glaucoma.
How does glaucoma affect vision?
In most people glaucoma will develop slowly, that is, it is chronic. Eventually the damage to the optic nerve will affect the peripheral part of vision. It will not affect the central vision where our reading, recognising faces and small detail goes on. There are blind areas in the 'side vision'. By the time this has occurred the damage to the optic nerve is advanced. The classic description of vision loss in glaucoma is 'tunnel vision'. In this chronic form there is rarely any pain.Although much less common, more of a concern is when the glaucoma is acute, that is it comes on very quickly. This often is painful and 'haloes' of light may be seen. Occasionally, abdominal pain and nausea may be present.
As glaucoma is preceded by a rise in IOP, then the best way to prevent glaucoma is by regular monitoring. One fortunate aspect for uveitis patients is that their intra-ocular pressures are likely to be monitored very regularly.
Glaucoma associated with uveitis
The inflammation that occurs with uveitis results in blood cell debris and 'sticky' protein leaking out of blood vessels into the clear, aqueous. This can lead to a rise in intra-ocular pressure in a number of ways:
Open Angle
The angle made between the iris and the cornea (see diagram 2 above) is normal or 'open'. However the trabecular meshwork, the drainage system through which the fluid in the eye escapes, becomes blocked by debris as a result of the inflammation. This results in a rise of intra-ocular pressure. This type is the most common and develops gradually.
Closed angle
There are two ways in which the angle is closed or narrowed.Posterior synechiae (see diagram 3 above)
Sometimes, as a result of the inflammation in uveitis, the iris sticks to the lens which is sitting close behind it. It may do so in isolated 'spots', but if extensive these posterior synechiae, may obstruct the flow of aqueous through the pupil and out through the drainage system (see diagram). The resulting rise in IOP, may be slow but it potentially can be very rapid if the iris becomes 'bowed' forward to 'close' the angle of the anterior chamber. As the angle is narrowed or closed it can be seen in the diagram that the drainage system will be become closed off.Anterior synechiae (not shown on diagram)
Sometimes the front surface of the iris becomes 'stuck' to the cornea or sclera. These anterior synechiae can also bow for ward the iris and close the angle.
Steroid Usage
Steroid drops used to treat uveitis sometimes cause the IOP to rise. This seems to happen in a minority of susceptible patients. This rise is usually gradual and normally occurs within a month or two of starting the drops, but can occur much later.Stopping or reducing the drops will lower the pressure, but eliminating inflammation, by vigorous treatment when necessary, is far more important in the long run and so the pressures are monitored and treated as necessary. The treatment of uveitis always involves this balance between treating vigorously to completely remove any inflammation whilst overall, using the minimum of drugs long term.
Other rare types:
Fuch's heterochromic uveitis in which a mild inflammation is associated with loss of pigment from the iris of the affected eye which becomes blue, if previously brown. Symptoms are often absent in the early stages but a raised pressure and cataract changes may occur later and affect vision.Posner Schlossman syndrome or glaucomatocyclitic crisis when the patient may see rainbow coloured haloes due to a sudden marked rise of eye pressure but the signs of uveitis are minimal and may be localised to the trabecular meshwork.
Rubeotic glaucoma, in which new blood vessels grow on to the iris, following retinal ischaemia. These vessels can block the trabecular meshwork.
Treatment of Glaucoma
As glaucoma is a risk factor to people with uveitis, the best approach is always prevention. The best means of preventing glaucoma are:- vigorous treatment of any inflammation to prevent the scarring and debris which is the commonest cause of the rise in intra-ocular pressure.
- Preventing the iris sticking to the lens (posterior synechiae). This is done with the use of mydriatic drops. Examples are tropicamide, cyclopentolate and atropine.
- Eye drops are all that are usually required. Examples are: betoptic, timoptol and trusopt. If you have difficulty using eye drops we have a Fact Sheet which will give you helpful guidance.
- Tablets may be used for more severe cases. A drug called diamox is used, usually for short spells.
- Laser. This usually involves a short, simple treatment which is carried out at the eye clinic. The aim is to open new channels fro the fluid to pass through.
- Surgery. If these treatments are unable to keep the pressures in the normal range, then the next stage may be surgery. The most common type of surgery is a procedure called a trabeculectomy. This involves cutting a small flap under the white of the eye, to allow a little fluid to escape and thus reduce the pressure.
Summary
- Glaucoma is damage to the optic nerve which can affect vision.
- Intraocular pressure (IOP) is the pressure within the eye and if raised for long, it can cause glaucoma.
- Up to 20% of people with uveitis may get glaucoma.
- Glaucoma may come on gradually (chronic) and have no symptoms, or it may, less often, come on suddenly (acute) and be painful and cause some loss of vision and possibly haloes of light are seen.
- Eye pressure must be monitored regularly when under treatment for uveitis and any sudden onset of symptoms suggesting an acute attack must be reported straight away.